
UTI During Pregnancy: Safety, Treatment And Prevention
Article by:

UTI during pregnancy is common. In fact, the risk of a UTI during pregnancy increases by up to 10%.
This is significant, as UTIs are already the most common bacterial infection, and a leading cause of doctor visits. And over the course of a lifetime, 50-60% of women will experience at least one urinary tract infection (UTI).
A UTI during pregnancy can increase the risk of complications, such as low birth weight and preterm labor. It can also lead to an increased susceptibility to infections in the child.
Asymptomatic bacteriuria (the presence of bacteria in the urine, in the absence of symptoms) is commonly seen in pregnancy, and is associated with increasing the risk of acute cystitis or kidney infection.
There are dietary and lifestyle changes that can be made to decrease the chances of a UTI during pregnancy, improve overall health and fertility, and also improve the health of any future children. I’ll expand on these more below.
Jump To Section:
- Why is a UTI during pregnancy more likely? >>>>
- How to minimize UTI during pregnancy. >>>>
- Can UTIs cause infertility? >>>>
- Complications caused by UTI during pregnancy. >>>>
- Treatment for UTI during pregnancy. >>>>
Why Is A UTI During Pregnancy More Likely?
The anatomical, biochemical, hormonal and other changes that occur naturally during pregnancy lead to an increased risk of UTIs, especially between 6 and 24 weeks gestation.
Hormonal changes alter the ureter tone and the movement of urine from the kidney to the bladder, otherwise known as peristalsis. This can lead to fluid stasis (a slow down or stoppage), increasing the likelihood of abnormal bacterial growth and infection.


The growing uterus puts physical pressure on the pelvic floor muscles, the bladder and the urethra. The extra pressure can result in the sensation of needing to urinate all the time, and it may feel more urgent.
Learn more about UTI and hormones in our expert video series.
Symptoms Of UTI During Pregnancy
Having a UTI during pregnancy can be a very stressful experience. It can also be difficult to know when you have a UTI, and what is considered ‘normal’.
New symptoms and feelings naturally accompany changes experienced during pregnancy. And these changes can occur on a daily basis.
Symptoms such as urgency, increased frequency and incontinence may be normal in pregnancy, but they may also be a sign of infection. It’s hard to know when to call your doctor or midwife.
There are many blogs and websites with information about pregnancy, but how do you know which information is credible?
Symptoms of increased urination and urgency tend to be worse during the first trimester and the later part of the third trimester. There are no guidelines on what is normal as far as frequency.
There are, however, other symptoms that may clue you in that you have a UTI.
If you have a UTI, you may experience:
- Painful or burning sensation while urinating
- Pelvic or lower abdominal pain or cramps
- Urgency when urinating
- Fever, chills or sweats
- Any vaginal or urinary bleeding
- Increased frequency of urination
- Cloudy or pink (blood) urine
- Strong-smelling urine
- Waking at night to urinate
- Change in the amount of urine, more or less
In addition to the above, a UTI may cause a strong urge to pee but then only a little comes out, pain during intercourse, tenderness in the bladder area or lower abdominal cramping.
You may notice your urine looks cloudy or mucousy or that there is blood in the urine or on the toilet paper when you wipe. There may be a strong or foul smell to your urine.
Factors That May Contribute To UTI During Pregnancy
When determining why some women get more UTIs, we need to consider both systemic issues, and issues localized to the bladder that may increase the risk of UTI.
Systemic issues may include:
- Immune issues
- History of repeat antibiotics
- History of other medication use
- Digestive health
- Diet
- Vitamin D levels
- Fluid intake
- Sexual activity
Local issues include the balance of the vaginal and bladder microbiomes at the time of conception, the presence of biofilms in the urinary tract, differences in anatomy and history of UTI.
When To See A Doctor For UTI In Pregnancy
 | “My first rule of thumb and one I teach every new mother, is to trust your intuition. If you think you have a UTI, call your doctor or midwife immediately. Being wrong is not the worst thing, and your doctor will understand.” |
If you suspect you have a UTI, it’s best to see your doctor or midwife as soon as possible.
They will do a urinalysis from a clean catch urine sample that you provide. This will determine whether there are white blood cells (WBCs), red blood cells (RBCs) and/or bacteria in your urine.
If the urinalysis comes back positive for WBCs and/or bacteria, your doctor should do a culture and antibiotic sensitivity test and prescribe a pregnancy safe antibiotic.
How To Minimize UTI During Pregnancy, By Preparing Beforehand
During the months prior to conception, it is important to prepare for pregnancy. This time is called the pre-conception time and it provides an opportunity to get as healthy as possible before conception.
Being healthy at the time of conception decreases the chances of complications during pregnancy and delivery, and increases the likelihood of a healthy child.
As females who have previously had a UTI are at increased risk of both UTI and asymptomatic bacteriuria in pregnancy, it is important to look at ways to decrease these risks prior to conception. One way to prepare is to improve the health of the digestive, bladder and vaginal microbiomes.
The Importance Of The Microbiome
The microbiome is a combination of bacteria, viruses, protozoa and fungi that live in our bodies. Different areas of the body have different combinations of organisms, and in a healthy state, these exist in balance.
Most research focuses only on the bacterial part of the microbiome. We know that the organisms that make up our microbiome help us digest our food, protect against infection, and produce vitamins.
Until recently, it was believed that the bladder was sterile. Recent research has shown us otherwise, and we now know that a urinary microbiome exists.
As we learn more about the human microbiome, we are beginning to understand on a deeper level which bacterial strains are beneficial and which are not.
Organisms that are commonly part of our normal gut flora, are also known to cause UTIs. Three such bacteria are Enterococcus spp and E. Coli, which are commonly found in the large intestine, and Group B Streptococcus, which is part of the intestines and the vaginal microbiome. Klebsiella is commonly found in the mouth and the respiratory tract.
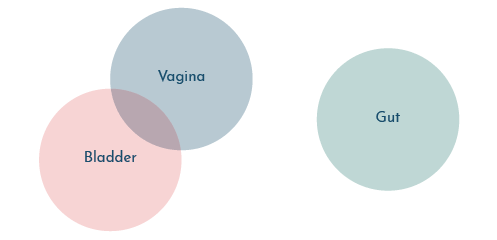
During pregnancy, changes occur to the urinary, vaginal and gastrointestinal microbiome, however, the impact of these changes are still under investigation. It is known, however, that the vaginal and urinary microbiomes are interconnected.
One point that does seem clear is that a higher number of certain Lactobacillus strains in your bladder may decrease the risk of UTI, while high levels of other Lactobacillus strains may increase the risk.
Studies show that it may be possible to alter the urinary and vaginal microbiome via the use of intravaginal probiotics and oral probiotics. Certain probiotics may decrease the risk of a UTI.
Can Diet Decrease The Risk Of UTI During Pregnancy?
Current research indicates that the gastrointestinal microbiome can be altered by diet, probiotic and prebiotic intake, prescription medication, including antibiotics, corticosteroids and H-2 blockers.
The effects of these medications on the bladder and vaginal microbiome are still being studied, but according to the information available, there may be an impact on these areas as well.
For those that have previously taken medications, probiotics and prebiotics during pregnancy may be beneficial.
Just a quick refresher:
Probiotics are beneficial bacteria that reside in the body and are generally known to provide health benefits.
Prebiotics are plant fibers that are not digested by the body, but instead pass through the digestive system to become food for beneficial bacteria.
Without sufficient prebiotics a healthy balance of the microbiome is unlikely.
There are two ways to get probiotics: Food, and supplements. Foods that naturally contain probiotics include sauerkraut, pickled vegetables, kombucha (with low sugar), tempeh, sourdough bread, miso, yogurt and kefir.
Making your own fermented vegetables, sourdough, kefir and kombucha is a good way to ensure any probiotics are still alive at the time of ingestion.
Prebiotics can be found in chicory root, Jerusalem artichoke, flax seeds, oats, garlic, onions, apples, and many other foods.
All bacteria, good and bad, feed on different things. What you feed your microbiome has a big impact on how healthy it is.
A varied diet that includes whole foods and lots of vegetables can promote a diverse and healthy gut microbiome during pregnancy and beyond. This in turn may lead to a reduced risk or recurrence of UTI.
Can UTIs Cause Infertility?
There are common bacterial strains that have been found in both the vaginal and bladder microbiomes. Sexual partners can also transfer bacteria back and forth during sexual contact.
Some of the bacteria already present, or transferred, can lead to infection while others will not.
In pregnancy, the microbiome changes, and this can heighten the susceptibility to a UTI.
Some bacterial strains can remain dormant for periods of time until the conditions are right to multiply. When this happens, infection can occur.
In addition to an increased risk of UTI, certain bacteria in the bladder, vagina and prostate can decrease the chances of conception. For instance, if a male has an overgrowth of certain bacteria, this can decrease sperm quality and motility.
These variables don’t just impact natural conception; they can also decrease the chances of success with IVF.
For all of these reasons, it’s important to maintain a healthy balance in both the bladder and the vagina prior to conception.
When Should You Test For UTI?
Experiencing a UTI at any time over the course of your life increases the risk of another UTI, including during pregnancy.
If you have had UTIs in the past, have frequent urination, or have been diagnosed with Interstitial Cystitis or chronic bladder pain, you may have bacteria in your bladder that can cause infection.
| “Many of my patients find that the nagging irritation they have in the bladder is really an infection, even after multiple negative urinalysis and cultures. It is important to identify these infections prior to conception.” |
As a UTI can lead to infertility, and in pregnancy can lead to serious complications, it is important to determine whether an infection is present, prior to conception.
Females with fertility issues may benefit from a urine test, while males with fertility issues may benefit from testing both the urine and semen.
There are specialized labs that can look more deeply at the bladder and vaginal microbiome to determine whether there are bacteria in the urine that should not be there.


Bear in mind though, that a negative dipstick and/or urine culture does not rule out a bacterial infection in the bladder.
If white blood cells (WBCs) are indicated on a dipstick, it is especially important to complete a urine test through a specialized laboratory. This is because the WBCs may indicate an infection that a dipstick or standard urine culture cannot detect.
| “As the screening urinalysis done during pregnancy may pick up asymptomatic bacteriuria, it is important to have this done. However, I am finding that the standard urinalysis and culture are missing many infections in the bladder. If a patient has any bladder symptoms but the standard tests come up negative, I suggest using next generation sequencing testing.“ |
If you discover you do have an infection, you can then treat it and repopulate a healthy microbiome before you try to conceive.
During pregnancy, if any symptoms indicate the presence of a UTI, testing should be sought immediately and antibiotic treatment used where necessary.
Complications Caused By UTI During Pregnancy
The presence of a UTI can increase the chances of complications during pregnancy, labor and delivery.
During pregnancy, the risks of untreated UTI include kidney infection, fetal growth restriction, preeclampsia and preterm birth.
Earlier, I briefly mentioned asymptomatic bacteriuria. This is a situation where there are no symptoms of a UTI, but a significant level of bacteria in the urine is present.
This is seen in about 10% of pregnancies. For this reason, there is generally a screening for asymptomatic bacteriuria at the first prenatal visit and again between 12 and 16 weeks.
Asymptomatic bacteriuria will be treated the same way a UTI is treated. When asymptomatic bacteriuria goes untreated in pregnancy, approximately 30% of patients will develop a symptomatic UTI. Up to 50% will develop a kidney infection.
Kidney infection in pregnancy is the leading cause of preterm labor, putting the baby at risk for serious complications and even death.
If a UTI is present during delivery, bacteria can get into the baby’s eyes, nose or mouth as they pass through the birth canal, causing infection.
The baby’s immune system is still developing at the time of delivery. A relatively harmless infection such as E. coli, the most common cause of UTIs, can be life-threatening in a newborn.
Treatment For UTI During Pregnancy
Given the risk of complications, treatment of a UTI during pregnancy is important. The preferred treatment is an antibiotic that is safe during pregnancy.
Natural treatments may help to prevent UTI, but once a UTI during pregnancy is identified, antibiotics are a more reliable approach.
| “I do not suggest using natural treatments when a UTI occurs during pregnancy. My approach is to use antibiotics to treat the infection then to use non-antibiotic therapies to provide additional and support to decrease the risk of negative effects from the antibiotics.” |
Antibiotics are categorized according to their potential risk to the baby. An antibiotic sensitivity test should be conducted to accurately identify which antibiotics are likely to be most effective.
Using this information, your doctor will provide the lowest risk antibiotics that will still be effective against the bacteria identified.
Antibiotics that are commonly used for UTI during pregnancy include:
- Cephalexin (Kephlex)
- Erythromycin
- Nitrofurantoin (Macrodantin
- Amoxicillin-Clavulanic acid (Augmentin)
- Fosfomycin (Monurol)
Different antibiotics are used in different trimesters. It’s important to take the prescribed antibiotics for the duration of treatment, usually 3-7 days, to reduce the risk of a recurrence.
Once you know you do not have an infection, you can consider other methods to help prevent a recurrence.
Prevention Of UTI During Pregnancy
Although there is very little scientific evidence to support behavioural recommendations around UTI prevention, some people find the following helpful:
- Always wipe front to back after urinating
- Urinate as soon as possible after having intercourse
- Wear cotton underwear and avoid thong underwear
- Do not use douches, scented feminine hygiene products, toilet paper or bath additives
- Eat a healthy, whole foods diet with lots of fruits and vegetables
- Take probiotics or eat foods high in probiotics
- Use a vitamin D supplement
- Take prebiotics, or foods high in prebiotics
- Drink adequate amounts of clear fluids
This last one is equally important during both pregnancy and lactation, as infants also need a lot of fluid.
Vitamin D levels appear to affect the vaginal microbiome during pregnancy. And although there is no direct link between vitamin D and the bladder, there is a link between the vaginal and bladder microbiome.
A basic rule for fluid intake in pregnancy is to drink half your body weight in ounces of water or clear fluids such as clear broth or herbal tea.
Prevention Of Yeast Infection During Pregnancy
There is an increased risk of yeast infection with both pregnancy and the use of antibiotics. So if you are pregnant and taking an antibiotic, your risk goes up exponentially.
Untreated yeast infection can lead to thrush in the newborn, so getting on top of any potential problems early is wise.
Probiotics, prebiotics, foods such as garlic, and a reduced sugar intake may be helpful in the prevention of a yeast infection.
The use of probiotics and prebiotics for the duration of the pregnancy may provide continued support. However, too much garlic may result in heartburn, so limiting any intake is generally preferred.
Yeast infection during pregnancy may also be treated with an antifungal.
A Case Study: The Link Between UTI And Fertility
Lisa came to me because she was having trouble conceiving. She had been diagnosed with infertility after 2 years of trying natural treatments, IVF and IUI. She had conceived twice, but lost both pregnancies.
We went through her history together. She mentioned she had a few UTIs in the past, but said they were no big deal. She also said at one point her doctors suggested she may have had Interstitial Cystitis. They then later told her she didn’t.
Lisa would wake up every night 2 to 3 times to use the bathroom. She didn’t consider this a problem because she was always able to get back to sleep.
Due to Lisa’s history with infertility and her urinary symptoms, I suggested a next generation sequencing urine test.
The test came back with 3 different pathogens. I recommended treatment for Lisa and used natural supportive therapies to help break up any biofilms present.
We then worked on Lisa’s diet, immune system and re-establishing a healthy microbiome. Within a year Lisa was pregnant.
Dr Deanna Berman’s Own Story
Dr Deanna Berman’s journey into natural medicine and her passion for helping women began with her own health issues, including Interstitial Cystitis.
Becoming a naturopathic doctor and midwife gave her the opportunity to study an integrative and functional approach to women’s health issues. When working with patients, Dr Berman uses the principles of naturopathic medicine, including: use the healing power of nature; treat the whole person; identify and treat the cause; first do no harm; doctor as teacher; and prevention.
Dr Berman understands both the necessity for medication and the limitations of natural medicine. She has found that the body has an amazing capacity for healing and recovery. Particularly when the obstacles to healing are removed and the body is given what it needs to heal.
After years of working with patients with chronic health issues, including chronic lyme disease and various autoimmune diseases, Dr Berman focused her practice on helping women with Chronic and Recurrent UTIs and Interstitial Cystitis/Painful Bladder Syndrome.
She will take the time necessary to research and understand the underlying causes. She takes an integrative approach to heal not only the bladder but the whole person.
You can learn more about Dr Berman on her website.
To get answers to commonly asked questions about chronic and recurrent UTI, visit our FAQ page. If you have any questions, you can leave a comment below or get in touch with our team.


Is there any information on your site about whether it is safe to try and get pregnant while dealing with recurrent/chronic UTI? My husband and I would like to try but I’m scared if I do end up pregnant that I will end up with serious complications as a result of this ongoing lowgrade infection that has persisted for a year plus. Any resources you can point me to or assistance would be most appreciated.
Hi Blanche, we have discussed pregnancy in some of expert videos on Youtube. Our interview with the late Professor Malone-Lee may be helpful. I hope it’s useful. Melissa
Can UTI cure completely when u use vitamin C
Hi Nalubega, we’ve covered vitamin c for UTI in more detail, and you may like to read that to learn more about why it may or may not help for some people. You can also get in touch directly, if you have questions. Melissa
Is it recommended to take biofilm dissolvers first, then antibiotics, or to take them together?
Hi Katarina, at the moment, there are no studies into the use of biofilm dissolvers for UTI, so if you’re interested in trying this approach, it’s best to speak with a practitioner that uses it. If you’d like to speak with Dr Deanna Berman, the author of this article, Details on how to get in touch with her can be found above. Melissa