
Recurrent UTI In Men: Prevalence And Causes
Article by:

Although much of our site is dedicated to recurrent urinary tract infection (UTI) in relation to female anatomy, recurrent UTI in men is not as uncommon as it may appear. Many of our community members are males who experience recurrent UTI, chronic bacterial prostatitis, or both.
As we know, the prostate is distinct from the urinary tract. However, the two are located right next to each other. For this reason, the prostate can play a role in increasing the risk of recurrent UTI in men. This is in addition to other risk factors, which we will expand on below.
Because it’s not always clear which organs are involved in lower urinary tract symptoms in males, getting an accurate diagnosis can be complicated.
Jump To Section:
- How Common Is Recurrent UTI In Men? >>>>
- Recurrent UTI In Men: Stages Of Infection >>>>
- The Role Of The Microbiome In Recurrent UTI >>>>
- Prostatitis And Recurrent UTI In Men >>>>
- Other Risk Factors For Recurrent UTI In Men >>>>
How Common Is Recurrent UTI In Men?
Although the majority of UTI diagnoses are in female patients, a significant number of males are also affected.
It’s sometimes easy to dismiss urinary symptoms as a normal part of life and getting older. However, urological conditions like UTI should be addressed. It’s important to get the information and support that is right for you.
First, let’s take a look at the stats…
- Approximately 20% of all diagnosed UTIs are in men.
- Around 13-14% of men will experience at least one UTI in their lifetime, compared with approximately 50% of women.
- At any one time, there may be 0.9-2.4 cases of UTI per 1000 in men younger than 55, and around 7.7 cases per 1000 in men over 85.
- In a study of male veterans, 1.46% reported having had a UTI within the past year. Nearly 15% of these cases were recurrences.
So, UTI in males is not as uncommon as you might think. And for some men it becomes a recurring illness.
Recurrent UTI has been defined as having experienced 2 distinct episodes of UTI in the last 6 months, or 3 in the last 12 months. But sometimes diagnosis is not straightforward.
IC, BPS, CP, CPPS… What Do They All Mean?!
Typical UTI symptoms can lead to a number of different diagnoses if experienced recurrently. We’ll break down some of the diagnoses most frequently received by male patients with recurrent symptoms.
Interstitial Cystitis Or Bladder Pain Syndrome
It is entirely possible, and more common than we’d like to think, for male patients to receive negative test results, even when they have symptoms of a UTI. To add another layer to the problem, for those who experience UTI symptoms recurrently and without a clear cause, it may lead to a diagnosis of interstitial cystitis (IC). This is also known as bladder pain syndrome (BPS).
This is what is called a diagnosis of exclusion. This means that IC/BPS is a term given to a group of symptoms for which a cause has not yet been found. IC is not a specific condition, and there is no test that can accurately result in this diagnosis.
Around 1.3% of men are estimated to be living with a diagnosis of IC (compared with 2.6% of women). Because of the inaccuracies of UTI testing, many of these may have been misdiagnosed.
Bladder vs. Prostate Symptoms
Other diagnoses which are commonly given when males present with ongoing urinary symptoms include chronic prostatitis (CP), or chronic pelvic pain syndrome (CPPS). There is likely to be some overlap between diagnoses of IC/BPS and CP/CPPS, because the symptoms are so similar. It’s not uncommon for different diagnoses to be given at different points in time.
The distinction here is that IC/BPS is thought to be localized to the bladder, and CP/CPPS to the prostate. But due to a lack of accurate testing methods, it can be difficult to get to the root of the problem. Precise diagnosis is complicated.
UTI testing inadequacies mean it is possible that when a patient is given a diagnosis of IC/BPS or CP/CPPS, they may in fact have a bacterial infection. This is despite tests returning negative results. Research has shown that in female patients with unexplained UTI symptoms, antibiotic treatment can be effective, indicating bacterial involvement.
Receiving one of the above diagnoses is not necessarily the end of the road for any patient. These diagnoses should be thought of as placeholders until the root cause is found.
Recurrent In Men: Stages Of Infection
The stages of infection in male UTI are very similar to the stages of infection in female UTI.
That said, the prostate can play an important role in the development of UTIs in men. But we’ll come back to this.
The ways in which UTI can become recurrent or chronic may also differ between male and female anatomy.
Animal studies have reported that males show a weaker immune response to UTI, possibly due to the role of androgen hormones. Males, as well as females with higher levels of testosterone, are more likely to be chronically ill with UTI for longer. Researchers suggest that more work is needed to better understand this diminished immune response, and the role of hormones.
As things stand, there is evidence to suggest that sex hormones may play a role in an initial infection escalating into a recurrent issue.
Chronic vs. Recurrent UTI In Men
Historically, it was generally understood that recurrent UTI occurs when bacteria causing an initial infection have been completely eradicated with treatment. And following on from this, new bacteria (the same or a different type) re-infect the urinary tract.
However, more recent evidence indicates that it is also possible for pathogenic bacteria to remain in the urinary tract after treatment. This can occur even when symptoms clear up. Symptoms of infection may then flare up again after treatment, as the bacteria once again multiply. This is commonly called chronic, or persistent UTI.
If symptoms return after treatment, it may be a sign that the original infection has not been effectively addressed.
How Does Infection Become Embedded In The Bladder?
Infection-causing (uropathogenic) bacteria can attach to the bladder wall and form a 3-dimensional community called a biofilm. You can think of this as a protective shield which may prevent antibiotics, or the body’s immune response, from reaching the bacteria inside.
Bacteria can also colonize within the bladder wall, forming what are known as intracellular bacterial communities (IBCs). IBCs have defense characteristics similar to biofilm, also making them difficult to treat. There is evidence for the involvement of both biofilms and IBCs in urinary tract infection, particularly for patients experiencing recurrent or chronic symptoms.
Bacteria residing within a biofilm are also more difficult to detect and may not be identified. This can be the case even with more sensitive testing methods. This means a prescribed antibiotic may not be appropriate for the bacteria present, even if it could permeate the biofilm.
Researchers are assessing different methods to address the bladder biofilm problem, including long-term antibiotic treatment protocols, biofilm disruptors, and fulguration.
We’ve covered biofilms in the bladder in more detail. A number of chronic UTI experts have also shared their insights on chronic bladder infection.
Clinical guidelines for recurrent UTI do not generally account for the possibility of an embedded infection. This is one of the reasons that recurrent UTI treatment often fails.
The Role of The Microbiome In Recurrent UTI
Discovering the underlying cause behind recurrent UTI in men can be complex. The reasons behind the development of this recurrent illness are different for every individual. There can be a number of contributing factors.
So let’s break down the key pieces to the puzzle.
We know that UTI is usually caused by bacteria. But it is possible that viruses, fungi and parasites may be involved in some cases. Because bacterial infection is by far the most likely cause, we’ll focus on this type of organism.
The Male Urinary Microbiome (MUM)
Compared to the microbiome of the gut, the bladder microbiome is much less dense. This is one of the reasons the bladder was previously thought to be sterile. Relatively recent advances in technology have allowed researchers to identify the presence of this sparse urinary microbiome in both males and females.
The urinary microbiome is the community of organisms living in the urinary tract. In healthy males, the urinary microbiome contains certain, usually harmless, bacterial species. These play a role in keeping the microbiome balanced.
The healthy female urinary microbiome also contains usually harmless bacterial species which maintain balance. But the species identified differ from those found in males.
The following outlines the bacteria that various studies have identified in the healthy male urinary microbiome, compared with the healthy female urinary microbiome:

**List compiled from multiple studies: Siddiqui et al. 2011, Wolfe et al. 2012, Hilt et al. 2014, Pearce et al. 2014, Thomas-White et al. 2016, and Karstens et al. 2016
Here is a representation of the distribution of most commonly found bacteria in male urine samples, according to Nelson et al. (2012):

The Urinary Microbiome During Infection
Interestingly, when a UTI is present, additional bacterial species and/or a higher amount of bacteria overall, are usually found in the urine. These are believed to be the cause of infection.
In both females and males, Escherichia coli (E. coli) appears to be involved in the vast majority of UTI cases (around 75% of cases) when standard cultures are used. According to one study, the following are the most common bacterial causes of UTI in men, after E. coli:
- Enterococci (21%)
- Proteus species (13%)
Klebsiella species, Pseudomonas species, and several types of Staphylococci and Citrobacter species are also sometimes found, but are less common.
Symptoms Related To The Urinary Microbiome
A study in 2018 aimed to find out more about the male urinary microbiome, and how the presence and abundance of different bacteria were connected to the symptoms experienced by male patients.
Although the study was run with a relatively small number of symptomatic patients (49), the researchers found detectable bacteria in 22% of men with mild UTI symptoms, 30% of men with moderate symptoms, and 57% of men with severe symptoms.
Bacteria were not detected in the remainder of samples. Although microbiota exist in both a healthy or imbalanced urinary microbiome, many testing methods are not sensitive enough to detect all bacteria present in a sample. This is especially true for bacteria in low abundance due to the absence of infection.
This was the first ever study to show a connection between the male urinary microbiome and severity of urinary symptoms.
Interestingly, the bacterial species Escherichia and Klebsiella were more likely to be found in male patients with moderate to severe UTI symptoms. And Streptococcus was very common in male patients experiencing severe symptoms.
The researchers used a urine testing method called Expanded Quantitative Urine Culture (EQUC). This method is able to detect more bacterial species than the standard urine culture test. Standard urine culture is strongly biased towards detection of E. coli.
Research has also been conducted on microbiome changes in chronic prostatitis (CP) / chronic pelvic pain syndrome (CPPS). A study using a symptoms scoring system found that the following bacteria were associated with particular reported experiences in men with CP/CPPS:

Although connections were found in this study between bacteria and reported symptoms, it is important to note that this research has not yet been replicated on a larger scale. More research is needed to clarify the specific bacteria associated with particular symptoms.
Prostatitis And Recurrent UTI In Men
The prostate can be linked to susceptibility to recurrent UTI in men, due to two issues in particular: benign prostatic hyperplasia and bacterial prostatitis.
Benign Prostatic Hyperplasia
Benign prostatic hyperplasia (BPH) occurs when the prostate gland increases significantly in size. BPH affects up to 60% of men over the age of 40. It is thought to occur due to hormonal changes.
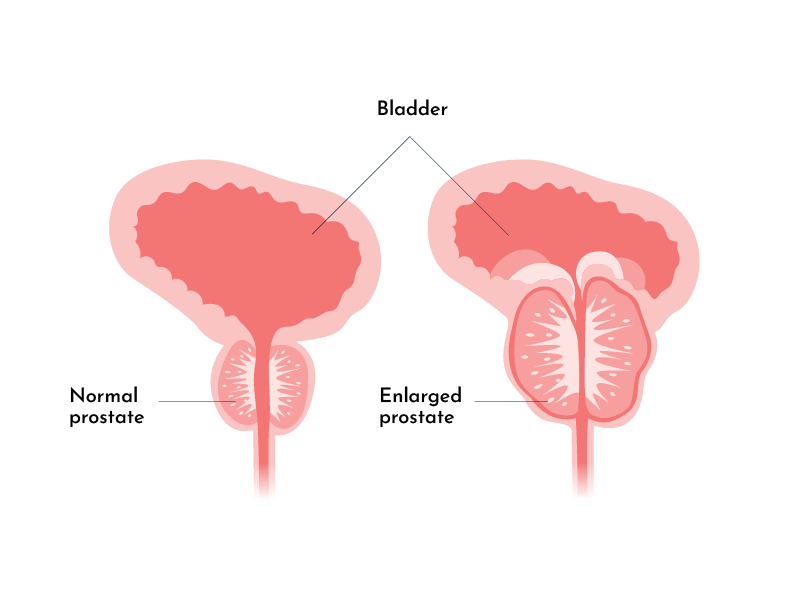
With BPH, the enlarged prostate pushes against the urethra (the tube carrying urine out of the body), making it more difficult to pass urine. This can result in symptoms such as difficulty urinating, difficulty fully emptying the bladder (bladder retention), and feeling the urge to pee more often than usual.
You might be thinking that these sound just like UTI symptoms, and they are. While BPH symptoms can be standalone, they might also indicate infection. If restricted urine flow means that the bladder is not emptying properly, bacteria in the urine have an opportunity to multiply and cause infection.
BPH also increases the risk of bladder trabeculation. This means a thickening of the bladder muscles as they work harder to move urine out of the body. As the bladder muscles become thicker and less elastic, the bladder stores urine for longer than usual. This increases the likelihood of urinary symptoms, as well as UTI.
BPH is not the only prostate-related risk factor for UTI; infection can also originate in the prostate and spread to the urinary tract, or vice versa.
Bacterial Prostatitis
Similar to UTI, prostatitis is more likely to affect older men. However, almost 50% of males will be diagnosed with prostatitis at some point in their lives.
Prostatitis as a general term can refer to acute / chronic bacterial prostatitis, chronic prostatitis / chronic pelvic pain syndrome (CP/CPPS), or asymptomatic inflammatory prostatitis.
For around 5% of those diagnosed, the diagnosis will refer to acute bacterial prostatitis, and 10% of these patients will later receive a diagnosis of chronic bacterial prostatitis or CP/CPPS.
The symptoms of bacterial prostatitis are very similar to those of UTI. But may also include pain in the lower back, rectum and/or perineum.
Some researchers have argued that bacterial prostatitis should be considered a type of UTI. This is because UTI and bacterial prostatitis patients exhibit similar symptoms. The bacteria causing the infection are also much the same.
E. coli is found in the majority of bacterial prostatitis cases, with Klebsiella spp., Pseudomonas spp., Proteus, Enterococcus spp. and Staphylococcus spp. also often found. And this is likely to be the case because the route of infection is the same: Uropathogenic bacteria climb the urethra and then colonize the bladder, kidneys and/or prostate.
Chronic Bacterial Prostatitis
As with infection in the bladder, prostate infection can also become chronic. The risk of chronicity increases with age as hormonal and structural changes occur.
The connection between recurrent UTI and chronic bacterial prostatitis (CBP) is significant as CBP is thought to be the most frequent cause of recurrent UTI in men (young to middle-aged). It has been found that for around 90% of men who develop febrile UTI (showing signs of fever), and 50% of men with recurrent UTI, there is some involvement of the prostate.
On the flip side, if an infection begins in the urinary tract, it can spread to the prostate. It’s possible for a reflux of urine to travel from the urethra to the prostatic ducts, transporting bacteria with it. Even if there is no infection in the urinary tract, ‘normal’ bacteria transported from the urinary tract may irritate the prostate.
Other Risk Factors For Recurrent UTI In Men
Some of the risk factors for recurrent UTI in men are the same as the main risk factors for UTI in women, These include sex, which we’ll move onto in a moment. For both biological sexes, risk factors include older age, catheter use, and a history of UTIs.
And as we’ve already seen, structural or functional changes, e.g. benign prostatic hyperplasia (BPH), as well as hormonal influences such as testosterone, can also pose a risk.
Conditions like prostate cancer, diabetes, Parkinson’s disease, multiple sclerosis and spinal cord injury can also act as risk factors for recurrent UTI in men. One reason for this is their role in ejaculatory dysfunction. Ejaculatory dysfunction includes retrograde ejaculation, where the bladder neck doesn’t contract as it should during ejaculation, allowing semen to enter the bladder.
Many of the treatments or surgeries used for lower urinary tract symptoms (LUTS) in males are also linked to ejaculatory problems. Surgical treatment for BPH in particular is associated with retrograde ejaculation.
It’s easy to see how the interconnectedness of the prostate and urinary tract adds complexity to a diagnosis. Successful treatment may require addressing issues in both.
Sex-Related UTI In Men
Even though UTI is not traditionally considered a sexually transmitted infection, pathogens (harmful bacteria or other organisms) can still pass between sexual partners.
Cases have been documented of couples who both test positive for significant levels of the same type of bacteria in their urine. Where further testing has been done, the same pathogens have been found in the prostatic fluid of men as in the vaginal secretions of their female partner.
Needless to say, there is evidence for sexual transmission of UTI-causing bacteria. This should be considered in cases where UTI appears to be exclusively linked to sex.
Urology specialist Dr. Malde has also advised that anal intercourse in particular can be a risk factor for UTI. With such close proximity, organisms in/around the anal area of your sexual partner can travel into your urethra.
It’s also important to note here that while one partner may experience symptoms of UTI related to a specific organism, the other partner may be asymptomatic even when the same organism is identified. For partners of the opposite sex, this may be due to the fact that the healthy urinary microbiome looks different in males and females.
If you suspect that bacteria are being transferred between you and a sexual partner, it may be helpful for both of you to get tested for UTI. STI testing will often also be recommended.
We’ve shared more information on how to prevent UTIs after sex, and you can learn more about the transmission of bacteria during sex from our discussion with recurrent UTI specialist, Dr. Tim Hlavinka.
On a final note, a question we get often is this: If I have a UTI, should I avoid sex?
Urinary symptoms in males may be made worse by having sex, because the infected area could become more irritated. For this reason, it may be safest to avoid sex until symptoms pass. Chronic UTI expert Professor Malone-Lee advises that there are ways to manage flare-ups caused by having sex.
What To Do Next?
Knowing the causes and risk factors for recurrent UTI in men is the first piece of the puzzle, and a very important place to start in terms of understanding how you can go about preventing a long-term issue.
It’s also extremely helpful to have a good understanding of the testing and treatment options available for recurrent UTI in men. This helps you find the most appropriate UTI management strategies for you.
If you have any questions, or would like to share your experience, you can leave a comment below or send us a direct message.



My 97 year old father has had a foley catheter for approx 4 years. Because symptoms are difficult to read with the foley, the last UTI landed him in the hospital for a week followed by a stay at rehab for 2 weeks. I’d be interested in knowing what he might do or supplements he might take to prevent infection.
Hi Janet, sorry to hear your father is experiencing that. We don’t have any resources specific to catheter use, however, you may find our interview on Hiprex useful. This therapy has been shown to be effective for prevention of UTI, and the clinician in the video briefly mentions she believes this is likely to be the case for catheter users as well. I hope this helps, Melissa
I am a 75 year old male and have had recurring UTIs since early December 2023 and still have sun and get blood in my urine despite being on antibiotics almost constantly. What should I do now?
Hi Alan, sorry to hear you’re experiencing that. Can you please get in touch and let us know where you are based? We’ll share any relevant resources we have. Thanks, Melissa
28 y/o M. Have been dealing with chronic prostate discomfort and recurrent prostatitis/uti for around 5 years. Doctors consistently tested me for STDs, always negative, when treated with diff antibiotics the symptoms subside for a while then come back. Not really painful urination (unless I’m very dehydrated) but will develop clear/ white discharge and prostatic/urethral pain and discomfort, foul smelling urine. Starting to lose hope that I can fully rid myself of this issue. This article was very informative and the most relatable I’ve read so far. Thank you
Hi Xavier, I’m sorry to hear this. I have emailed you, Molly.
My husband had the same symptoms with Xavier. Except that he was newly diagnosed with UTI. Had his first course of antibiotic, results came back clear and then after 2 weeks He started to have the same symptoms again so Doctor treated him for STD without being tested. Thank you for this very informative article.
Hi Len, I’m sorry to hear this. I have emailed you some information about negative test results. I hope it helps, Molly.
I had a severe UTI in December 23′ which lasted over 5 days. In some instances, the infection was so severe I was passing urine every 5 minutes and unable to sleep at night time. The first course of antibiotics did not seems to help leading my GP to prescribe me a stronger dosage. This cleared the UTI however after several weeks I experienced a strong odder first thing in the morning (did not smell the rest of the day) and the infection came back (not as severe). I have just finished by fourth different type of anti-biotic and the infection seems to be coming back albeit it not as severe. Would you have any advise?
Hi Paddy, I’m sorry to hear this. I have emailed you, Molly.
I have been with dealing similar UTI symptoms for around the same time period. I have taken multiple courses of antibiotics only for the UTI to come back after a few weeks but less severe. Please advise. And thank you for this article.
Hi Patrick, I’ve sent you an email with some information. Best wishes, Issy
husband (76yo) had lumbar surgery in jan2023. “supposedly” developed UTI mid-Feb(was hospitalized one week). On 4/1 started urinary incontinence, vomitting, elevated temp, overall very weak & much difficulty walking & with balance(while using walker). Now being told it is a UTI again. Has not been seen by surgeon since OR on 1/11/23.
Hospital says he is out on Medical Leave! PC trying to deal with this!!!!
Hi Geraldine, I’ve just sent you an email with more information. I hope it helps, Melissa
I had a bad UTI around 15 years ago, which kept reoccurring, mostly with mild symptoms. after scans, CTs, endoscopy, etc urologist found nothing and uti seemed to go away. Subsequently, during Medicals, uti detected and a few times more painful. Various antibiotics and a couple more scans found nothing. Now for circa 9 months persistent uti with regular urologist visits and test – apart from some scaring to kidneys nothing. After antibiotics uti returns in 3-4 days, always ecoli. tried low dosage twice for circa 2 months. Only unusual symptom is on antibiotics 1st & 3rd wee in morning clear, 2nd wee cloudy. Next options seem to long term low dosage or live with it. Both have risks.
Hi Steven, sorry to hear you’re experiencing that. If you have any questions you’re always welcome to get in touch directly. We’ll do what we can to help. Melissa